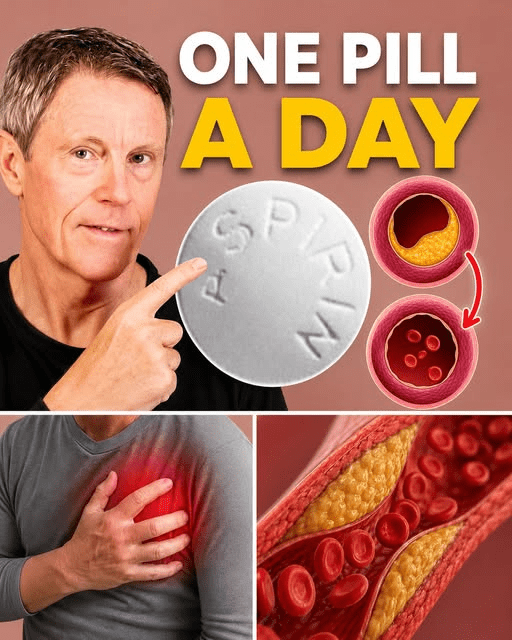
For decades, it was the gold standard. You reached age 60, and like clockwork, you started taking a daily baby aspirin. It was the ultimate “just in case” insurance policy for your heart. But recently, the rules changed, leaving millions of us wondering: Is my daily habit actually protecting me, or is it putting me at risk?
If you’ve been feeling conflicted about those 81mg tablets, you aren’t alone. Even the experts at the US Preventive Services Task Force shifted their stance in 2022. The truth is, aspirin isn’t a “one size fits all” vitamin—it’s a powerful tool that requires a bit of strategy to use safely.
The “Snot” in Your Arteries: Why We Take It
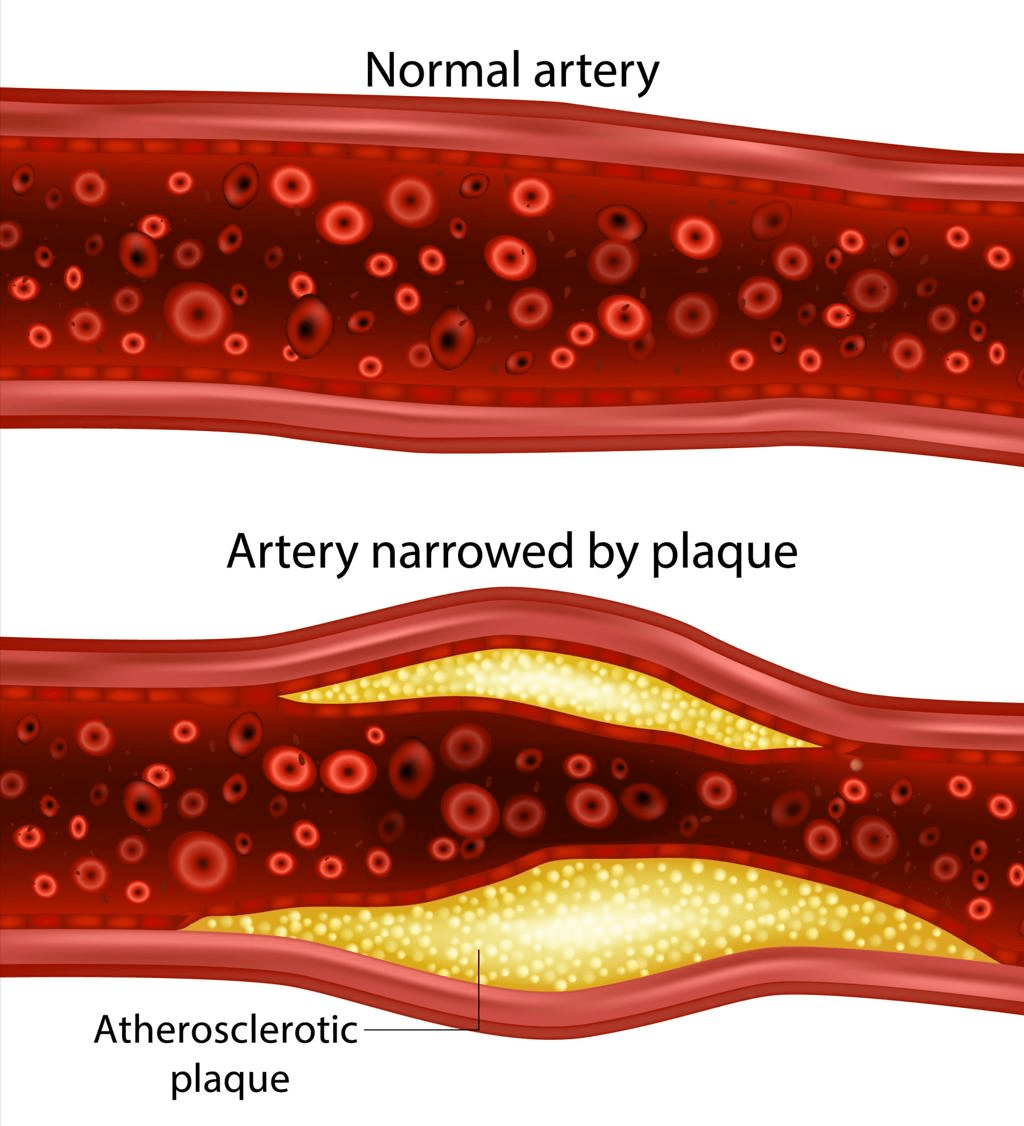
To understand if you need aspirin, you have to understand what it’s actually fighting. Most people think of arterial plaque as hard, waxy buildup—like old grease in a pipe.
But the dangerous plaque is actually more like “goop” or mucus. When this inflamed “snot” triggers a reaction, your blood’s platelets rush in to form a lattice. If that lattice gets too big, it creates a clot. That’s the moment a “coulda, shoulda, woulda” prevention story turns into a heart attack or stroke.
Aspirin works by making those platelets “slippery” so they can’t stick together.
The Great 2022 Shift: Primary vs. Secondary

The reason the guidelines changed comes down to two words: Primary and Secondary.
- Primary Prevention: You have no known heart disease or visible plaque, but you take aspirin “just because” you’re over 60. The new verdict? For most healthy seniors, the risk of internal bleeding (especially in the gut or brain) now outweighs the heart benefits.
- Secondary Prevention: You already have evidence of plaque (found via a scan) or you’ve had a previous cardiac event. The verdict? Aspirin is still a literal lifesaver here.
The “Juice” Rule: For healthy adults over 64 with no signs of disease, the “juice” (protection) is no longer worth the “squeeze” (bleeding risk).
3 Times Aspirin is NOT the Answer
Many people assume aspirin is the “universal blood thinner,” but there are specific situations where it fails to do the job:
- Atrial Fibrillation (A-Fib): If your heart has that “flopping fish” feeling, aspirin is often ineffective at preventing strokes caused by A-Fib. These clots are different and usually require prescription “NOACs” like Eliquis or Xarelto.
- The “Stress Test” Trap: Don’t rely on a normal stress test to decide if you need aspirin. A stress test only catches blockages over 50%. Since most heart attacks happen in arteries with less than 50% blockage, you could “pass” the test while still carrying dangerous, unstable plaque.
- True Aspirin Allergies: If you have a history of GI bleeds or allergies, even a baby aspirin is off the table.
Natural Support for “Slippery” Blood

If you aren’t a candidate for daily aspirin, or you want to support your vascular health naturally, the earth provides some remarkable alternatives. These don’t replace medical advice, but they are staples in a preventive lifestyle:
- Omega-3 Fish Oil: Think of this as “teflon” for your blood cells. It reduces the stickiness of platelet membranes.
- Nattokinase: A potent enzyme derived from fermented soy that specifically helps break down fibrin (the “mesh” of a clot).
- Turmeric & Ginger: Both contain natural compounds that inhibit platelet activation, similar to how aspirin works, but with a much gentler profile for the stomach.
- Garlic: High doses of aged garlic extract have been shown in studies to help stabilize that dangerous “soft plaque” so it doesn’t rupture in the first place.
The Bottom Line
Don’t just stop or start a regimen because of a headline. The real “secret” is knowing your own body. If you’re over 50, ask your doctor about a CIMT (Carotid Intima Media Thickness) test. It’s a simple, non-invasive ultrasound that looks for that “goop” before it becomes a problem.
If you have the plaque, the aspirin is likely your best friend. If your arteries are clean, you can probably skip the pills and focus on the lifestyle.
Have you changed your aspirin habit recently? Let’s talk about it in the comments—I’d love to hear your experience.