The real truth about blood pressure targets for older adults might surprise you. Imagine this: You’re in your doctor’s office, feeling proud that your numbers finally hit that “perfect” 120/80 mark. Your physician smiles, congratulates you, and says you’re doing great. But later that night, you stand up too quickly—and the room spins. Your heart races, your vision blurs, and you grab the wall to avoid falling. What if that celebrated “success” is quietly putting you at greater risk?
For years, the standard advice has been clear: Get blood pressure under 130/80, ideally closer to 120/80, to protect your heart, brain, and kidneys. This makes perfect sense for younger adults in their 40s, 50s, or even early 60s. Lower numbers in midlife dramatically cut risks of heart attacks, strokes, and long-term damage. But as we cross into our 70s and beyond, something shifts. The body changes in ways that make aggressive lowering potentially harmful rather than helpful.
Why Standard Targets Can Backfire After 75
Picture Margaret, a lively 78-year-old who loves gardening and visiting her grandkids. Her blood pressure hovered around 145/85. Her doctor, following guidelines, added medication after medication until it dropped to 122/76. At first, she felt fine. Then came the dizziness—especially in the mornings or after meals. One day, it led to a nasty fall in the kitchen, fracturing her hip. Months of pain, rehab, and lost independence followed. Margaret’s story isn’t rare; it’s a pattern seen far too often.
The issue? When blood pressure drops too low in older adults, it can cause orthostatic hypotension—a sudden plunge when standing. This starves the brain of blood flow momentarily, triggering lightheadedness, fainting, or falls. Research highlights that very low readings increase serious fall risks by up to 28% and link to higher overall mortality in some groups.
Aging brings three key changes:
- Arteries stiffen like an old garden hose losing flexibility. They need slightly higher pressure to push blood effectively to the brain and organs, especially against gravity.
- Baroreceptors—pressure sensors in blood vessels—become less responsive. They react slower to position changes, making sharp drops more likely if baseline pressure is already low.
- Medications linger longer due to slower kidney and liver function. A dose fine for a 50-year-old can overshoot in someone 75+, pushing pressure dangerously low.
These shifts explain why “one-size-fits-all” targets from middle-age studies don’t always apply later in life.
What Recent Research Really Shows
Large studies tracking thousands of seniors reveal a nuanced picture. While very high pressure (over 150 systolic) raises stroke and heart risks, very low pressure (below 120) often correlates with more problems like falls, kidney issues, and sometimes worse survival.
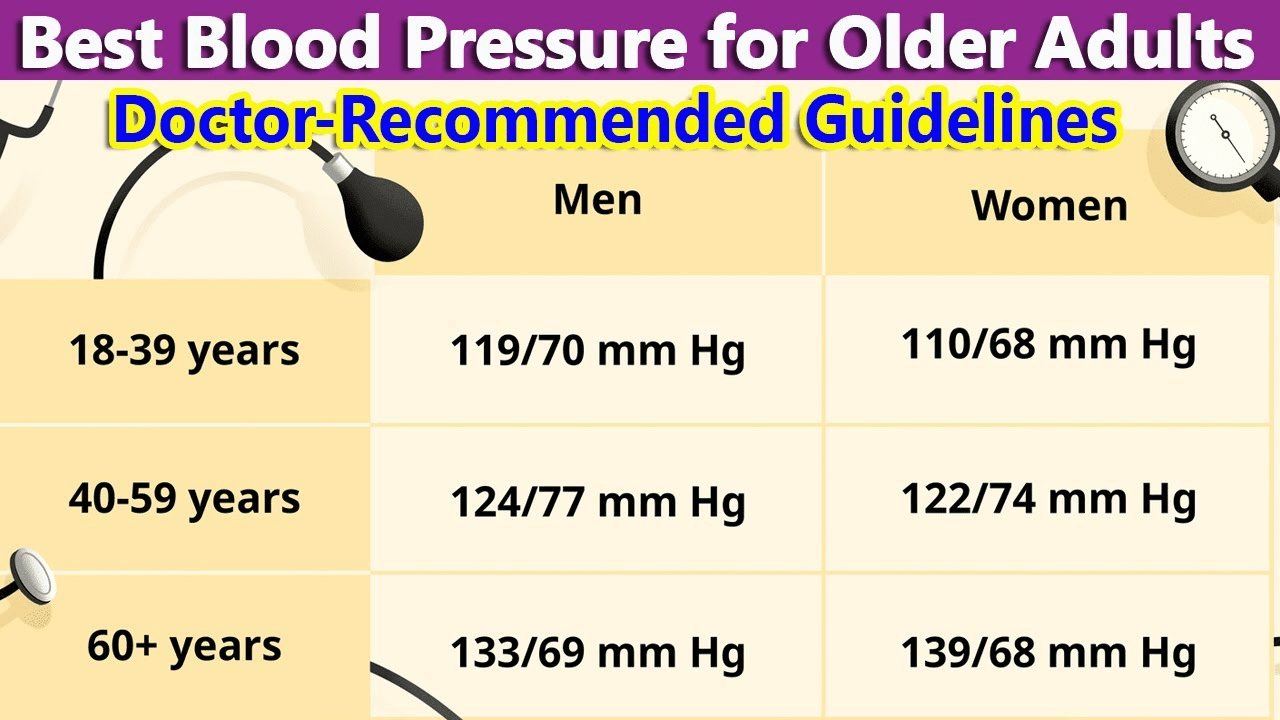
In key analyses, the sweet spot for many over 75 appears higher than traditional guidelines suggest—often around 130-145 systolic for healthier individuals, adjusting upward for frailty. This range balances heart protection with avoiding perfusion issues to vital organs.
But wait—there’s more. Major trials like SPRINT showed benefits from intensive control (target <120) even in those 75+, reducing cardiovascular events and mortality without dramatically spiking falls in carefully monitored settings. Other evidence points to individualized approaches: Frailer adults or those with multiple conditions may fare better with relaxed targets to prevent side effects.
The bottom line? Aggressive lowering helps many, but not everyone. Pushing too low can trade one risk (cardiovascular) for another (falls, injury).
The Hidden Danger: Orthostatic Hypotension
Have you ever felt woozy standing up? That’s often orthostatic hypotension in action. It affects many seniors on blood pressure meds, yet it’s frequently overlooked.
Here’s a simple home test that could change everything:
- Lie flat for 5 minutes and measure your blood pressure.
- Stand immediately and measure again right away.
- Note any drop: A systolic fall over 20 mmHg or diastolic over 10 mmHg signals a problem.
If this happens, even with “great” sitting numbers, it means upright posture starves your brain. Repeated episodes raise fall odds dramatically.
John, 82 and active until recently, ignored mild dizziness. His pressure was 118/70 sitting. Standing? It plummeted to 92/58. After one bad fall, he adjusted meds with his doctor—raising his target slightly—and regained confidence.
Finding Your Personalized Target
Guidelines evolve, but current evidence supports tailoring:
- For healthier adults 65-74: Often aim for under 140, potentially 130-140 systolic.
- For 75-84, relatively fit: 135-145 may offer the best balance.
- Over 85 or frail: 140-150 often prioritizes quality of life and fall prevention.
Diastolic ideally stays above 65-70 to support heart filling. Always factor in conditions like diabetes or heart history—130-135 might suit some high-risk cases.
Home monitoring beats office readings. Track morning and evening averages over weeks for the true picture.
Practical Steps to Take Control Safely
Ready to act? Start here:
- Get a reliable home monitor — Affordable and accurate ones are widely available.
- Log readings consistently — Same time daily, note symptoms.
- Do the orthostatic test weekly — Especially if on meds or feeling off.
- Talk openly with your doctor — Share logs, symptoms, and ask: “Given my age and health, what’s my ideal range?”
- Review medications — Never stop abruptly, but discuss adjustments if side effects appear.
- Adopt supportive habits — Rise slowly, stay hydrated, eat small frequent meals, consider compression stockings if advised.
These steps empower you without overhauling everything overnight.
Common Myths Debunked
You might think: “Lower is always better.” Not necessarily past 75—balance matters.
Or: “If I feel okay, my numbers must be fine.” Symptoms like fatigue or fog can signal subtle under-perfusion.
Research evolves slowly into practice. Many doctors follow older guidelines, so bring fresh questions to appointments.
Empowering Your Health Journey
Understanding this nuance shifts you from passive patient to informed partner in care. You now know why 120/80 isn’t universally ideal, how orthostatic drops sneak up, and why personalized targets save more than just numbers—they preserve independence.
The potential? Fewer scary falls, sustained energy, and peace of mind knowing your approach fits you.
This article is for informational purposes only and is not a substitute for professional medical advice. Blood pressure management should always be individualized. Consult your healthcare provider before making any changes to medications or targets.